I’ve been writing a bit about supported self-management over the last few months. Partly because it’s topical given that medications and exercise offer very small reductions in pain and disability, and people do have lives outside of swallowing a pill and doing 3×10 reps! And partly because it is what we end up doing. It is the bulk of what people living with pain use to have lives.
Self-management refers to a broad range of strategies people with pain use in their daily lives to help them live well. I’m aware of the multiple definitions that exist for self-management, and that the level of agreement isn’t great – and of course, throughout my discussion I always consider self-management to be supported. Supported by relationships with health professionals, friends and family, and within healthcare systems. Or perhaps not so much the latter.
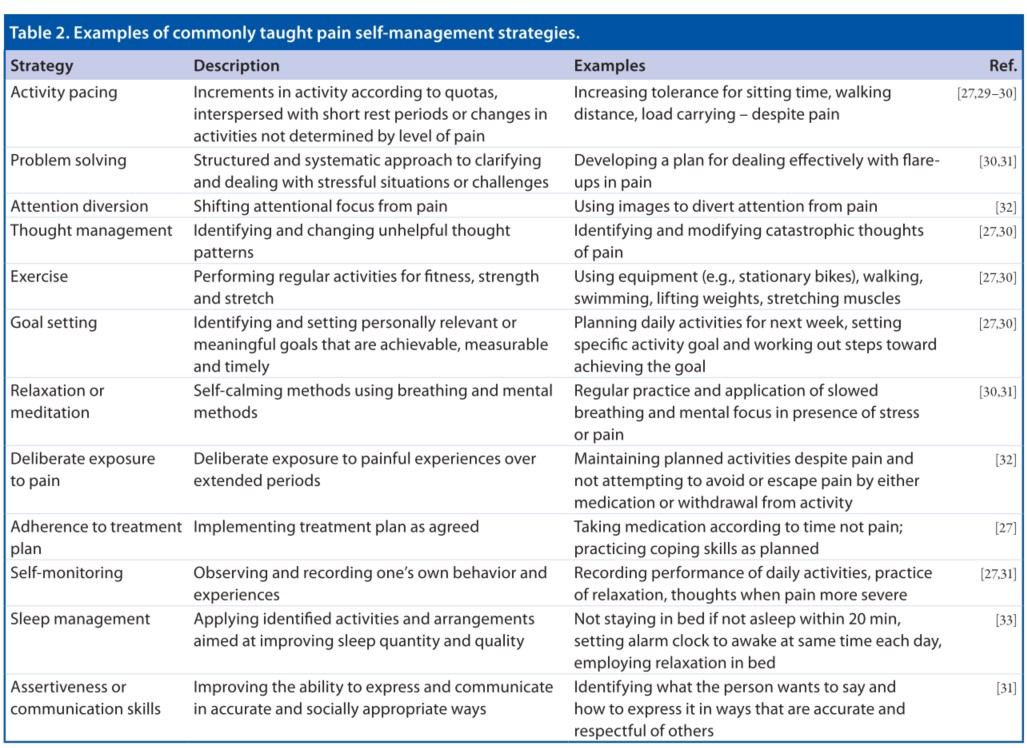
Drawing on Nicholas & Blyth’s commentary from 2016 (because it’s pretty good), the key elements of self-management are:
- being actively involved in daily actions to manage the effects of pain
- knowing about pain and the options for managing pain
- monitoring signs and symptoms and responding to these
- collaborating with health professionals and others to develop ways of living around pain
From my perspective, some of the things that seem to be important in self-management are:
- Knowing how to set limits on demands/obligations from others. This is important because, whether we like it or not, pain does limit how much we can do. I’m not certain this is always considered, especially when I hear of people with pain being asked to do far more than I am expected to do. It is reasonable for people with pain to say no! Being able to say no shouldn’t come with a host of negative consequences like ‘you’re being noncompliant’, or ‘you’re not trying hard enough’, or ‘you’re just using our pain as an excuse to get out of things.’ Unfortunately, for those with an accident insurance claim, the consequences of saying no can be pretty harsh.
- Knowing how to adapt, adjust, tweak or vary anything being suggested. This includes mindfulness, exercise, medications, pacing… And this one is a doozy because there are some very shouty people who think that their way to [insert strategy here] is The Way. If we had agreement we’d all be seeing good results, right? We don’t, and we see so many different ways of doing [insert strategy here] that I think we can be pretty confident that there is no One Way to do any of them. Contextual sensitivity is needed. What this means is being able to adapt, adjust, tweak or vary the things to suit the purpose and the context. “How it functions in this context” is likely more important than “what it looks like in a healthcare context”.
- Being able to feel the effect. To know what it feels like, and use this as the guide for action. No I don’t mean only the short-term effects (resting does feel great at times) but over the longer term. Asking: Does this [insert strategy here] give more options, allow me to move towards the things that matter, adapt and adjust over time? Helping someone feel what it feels like so they can use that ‘body knowledge’ in any context probably means less talking from the therapist, and more guiding to notice and reflect. Now that’s a set of skills many therapists have never been taught, particularly movement therapists.
I’ve written before about the way ‘the social’ is often ignored in a ‘biopsychosocial’ approach to pain. The factors that fall into the social are the very ones those of us living with chronic pain most have to deal with. The social impacts on how much we’re listened to by health professionals and others, whether we can say no without harsh consequences, how OK it is to adapt, adjust, tweak or vary how we do anything (including the things clinicians suggest), how much notice we take of our own body (because we’re often being talked at, taking our attention away from what we’re actually experiencing), and even on whether we can get to have a decent sleep (I am that person sneaking away from a social event and snuggling down in my bed at 9.30pm!).
Social factors also popularise what’s on offer, how much these things cost, who is able to offer them, and whether they fit in our lifestyle. Our gender, age, ethnicity, cultural background, religion, socio-economic status, education, the type of work we do – all of these are social. And they make an extraordinary difference to how we can employ self-management. A study by Webster et al., (2022) examined what people with chronic pain do in their health work in the context of having difficulty making ends meet.They found there is work in managing chronic pain alongside poverty and subsistence, trying to legitimise their needs (and themselves), attempting to adhere to biomedical models (even when it is clear that social contextual factors are hugely contributing), and navigating multiple diagnoses. The authors call this ‘chronic struggle’ – a term that resonates with my experiences listening to people with chronic pain as a clinician. The experiences they describe are ‘the social’ – and clinicians, we need to listen.
If you’re working in a supermarket job, you can’t just stop the queue of people at the checkout to go do a stretch and pace yourself. The skills needed to make that happen are in those three self-management skills: to safely say no, to be able to adapt (etc), and to use how it feels to guide actions. The social aspects of doing self-management take grit, confidence, great communication skills, and quite a lot of personal power. And for many people with chronic pain, being assertive and taking control over what is expected from you is high risk.
The social is about participation, if you’re going to use ICF (WHO – ICF). Participation is all about being able to do the things – in ICF-speak it’s “… involvement in a life situation… Participation restrictions are problems an individual may experience in involvement in life situations.” and goes on to say “…Because the current environment brings in a societal context, performance as recorded by this qualifier can also be understood as “involvement in a life situation” or “the lived experience” of people in the actual context in which they live.”
Self-management, because it is about daily life, is inevitably about participating in life situations. It’s up to health professionals to learn about a person’s real daily life contexts to make sure that what is suggested as ‘self-management’ can actually be done, and to help people with pain develop those three skills I’ve suggested at the very least. And for all of us to push back on attempts to limit our ability to do those without kickbacks.
Nicholas, M. K., & Blyth, F. M. (2016). Are self-management strategies effective in chronic pain treatment? Pain Management, 6(1), 75-75–88. https://doi.org/https://doi.org/10.2217/pmt.15.57
Webster, F., Connoy, L., Sud, A., Rice, K., Katz, J., Pinto, A. D., Upshur, R., & Dale, C. (2022). Chronic Struggle: An Institutional Ethnography of Chronic Pain and Marginalization. J Pain. https://doi.org/10.1016/j.jpain.2022.10.004